
Ventilator settings are ordered by the physician and are individualized for each patient. Ventilators are designed to monitor many components of the patient’s respiratory status. Various alarms and parameters can be set to warn healthcare providers that the patient is having difficulty with the settings.
Respiratory Rate (RR)
The respiratory rate is the number of breaths the ventilator delivers to the patient each minute. The rate chosen depends on the tidal volume, the type of pulmonary pathology, and the patient’s target PaCO2. The respiratory rate parameters are set above and below this number and the alarm will then sound if the patient’s actual rate is outside of the desired range.
(The following are guidelines.) For patients with obstructive lung disease, the rate should be set at 6-8 breaths/minute to avoid the development of auto-PEEP and hyperventilation, or “blowing off CO2”. Patients with restrictive lung disease usually tolerate a range of 12-20 breaths/minute. Patients with normal pulmonary mechanics can tolerate a rate of 8-12 breaths/minute. The patient should be monitored on the initial rate setting and adjustments made as necessary.
Tidal Volume (VT)
The tidal volume is the volume of gas the ventilator delivers to the patient with each breath. The tidal volume parameters are set above and below the desired number, and the alarm will sound if the patient’s actual tidal volume is outside of the desired range. This is especially helpful if the patient is breathing spontaneously between ventilator-delivered breaths, since the patient’s own tidal volume can be compared with the tidal volume delivered by the ventilator.
The usual setting is 5-15 cc/kg, based on compliance, resistance, and type of pathology. Patients with normal lungs can tolerate a tidal volume of 12-15 cc/kg, whereas patients with restrictive lung disease may need a tidal volume of 5-8 cc/kg.
Fractional Inspired Oxygen (FiO2)
The fractional inspired oxygen is the amount of oxygen delivered to the patient. It can range from 21% (room air) to 100%. It’s recommended that the FiO2 be set at 1.0 (100%) upon the initiation of mechanical ventilation to allow the patient to get used to the ventilator without experiencing hypoxia. However, 100% oxygen should not be used continuously for long periods of time because of the risk of oxygen toxicity. Oxygen toxicity causes structural changes at the alveolar-capillary membrane, pulmonary edema, atelectasis, and decreased PaO2. Once the patient is stabilized, the FiO2 can be weaned down based on pulse oximetry and arterial blood gas values. The FiO2 should only be as high as is necessary to keep the PaO2 in the desired range.
Most ventilators have a temporary 100% oxygen setting that delivers 100% oxygen for only a few breaths. This should always be used prior to and after suctioning; during bronchoscopy, chest physiotherapy, or other stressful procedures; and during patient transport.
Inspiratory: Expiratory (I: E) Ratio
The I: E ratio is usually set at 1:2 or 1:1.5 to approximate the normal physiology of inspiration and expiration. Occasionally, a longer inspiratory than expiratory time is desired to allow more time to oxygenate the patient’s lungs. This is called inverse ratio ventilation, and will be discussed later.
Pressure Limit
The pressure limit regulates the amount of pressure the volume-cycled ventilator can generate to deliver the preset tidal volume. Because high pressures can cause lung injury, it’s recommended that the plateau pressure not exceed 35 cm H2O. If this limit is reached, the ventilator stops delivering the breath and alarms. This may be an indication that the patient’s airway is obstructed with mucus, in which case, the high pressure is usually resolved with suctioning. It can also be caused by the patient coughing, biting on the ETT, breathing against the ventilator, or by a kink in the ventilator tubing.
Flow rate
The flow rate is the speed with which the tidal volume is delivered. The usual setting is 40-100 liters per minute.
Sensitivity/Trigger
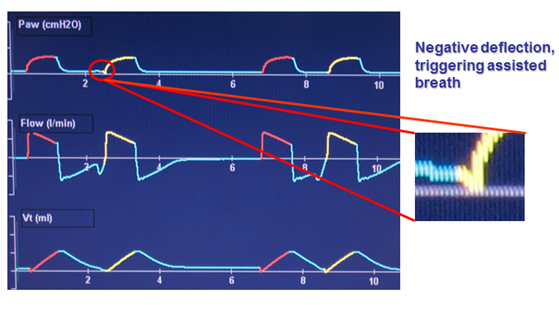
The sensitivity determines the amount of effort required by the patient to initiate inspiration. It can be set to be triggered by pressure or flow. Flow triggering is a better setting for patients who can breathe spontaneously because it reduces the work of breathing.
Sigh
The ventilator can be programmed to deliver an occasional sigh with a larger tidal volume. The use of frequent sighs was popular during the 1970s because it was thought that it prevented collapse of the alveoli (atelectasis), which can result from the patient constantly inspiring the same volume of gas. However, recently there has been concern that the increased pressure produced in the alveoli may heighten the risk of the alveoli rupturing and causing pneumothorax.
Ventilator Settings summary that nurses deal with the most
|
S.No. |
SETTING |
FUNCTION |
USUAL PARAMETERS |
|
|
Respiratory Rate (RR) |
Number of breaths delivered by the ventilator per minute |
Usually 4-20 breaths per minute |
|
|
Tidal Volume (VT) |
Volume of gas delivered during each ventilator breath |
Usually 5-15 cc/kg |
|
|
Fractional Inspired Oxygen (FiO2) |
Amount of oxygen delivered by ventilator to patient |
21% to 100%; usually set to keep PaO2 > 60 mmHg or SaO2 > 90% |
|
|
Inspiratory:Expiratory (I:E) Ratio |
Length of inspiration compared to length of expiration |
Usually 1:2 or 1:1.5 unless inverse ratio ventilation is required |
|
|
Pressure Limit |
Maximum amount of pressure the ventilator can use to deliver breath |
10-20 cm H2O above peak inspiratory pressure; maximum is 35 cm H2O |
Modes of mechanical ventilation
Modes of mechanical ventilation are described by the relationships between the various types of breaths and by the variables that can occur during the inspiratory phase of ventilation. Each mode of ventilation is distinguished by how it initiates a breath (trigger), how it sustains a breath (limit), and how it terminates a breath (cycle); these are referred to as phase variables.
The best mode of mechanical ventilation is the one that provides maximum therapeutic benefit with the fewest side effects. Mode selection and individual ventilator settings are geared towards the patient’s diagnosis and history as well as integrated data from laboratory, radiology and physical examination.
Basic modes of ventilation
1. Continuous Mandatory Ventilation (CMV)
2. Assist Control (A/C) Ventilation
3. Intermittent Mandatory Ventilation (IMV)
4. Positive End Expiratory Pressure (PEEP)
5. Continuous Positive Airway Pressure (CPAP)
Continuous Mandatory Ventilation (CMV)
· CMV completely controls the patient’s ventilation. The ventilator provides a mechanical breath on a preset timing. Patient respiratory efforts are ignored.
· This is generally uncomfortable for children and adults who are conscious and is usually only used in an unconscious patient.
· In this mode the ventilator delivers a mechanical breath with pre-set volumes at a pre-set rate and a pre-set flow rate.
· The patient CANNOT generate spontaneous breaths, volumes, or flow rates in this mode.

Fig: Diagram shows display of volume, flow and pressure waveforms as seen in the CMV mode. The shaded areas marked with “E” represent the expiratory phase.

Disadvantage
The major disadvantage of CMV is that it is not synchronized with the efforts of the patient. When the patient is “out of sync” with the ventilator, he attempts to exhale as the ventilator is in the inspiratory phase. As a result, airway pressure builds to abnormally high levels and the remainder of the inspiratory volume is not delivered. This “bucking” causes a high-pressure alarm. Signs and symptoms of ventilator dys-synchrony include:
• Agitation
• Diaphoresis
• Tachycardia
• Tachypnea
• Paradoxical thoraco-abdominal breathing pattern
• Increased PIP (peak inspiratory pressure)
Assist Control (A/C) Ventilation
· The A/C mode is similar to CMV, but it allows the patient to trigger an assisted breath at any time.
· A/C delivers the pre-set volumes at a pre-set rate and a pre-set flow rate in response to the patient’s own inspiratory effort, but will initiate the breath if the patient does not do so within the set amount of time.
· The patient CANNOT generate spontaneous volumes, or flow rates in this mode. All delivered breaths, whether mandatory or patient-triggered, will be delivered by the ventilator according to the set parameters. i.e. All breaths in the assist-control mode receive the same FiO2 and tidal volume.
· Hyperventilation and respiratory alkalosis may result from occurrences that increase the patient’s spontaneous rate such as anxiety or neurological factors. A high sensitivity setting that causes the machine to cycle too frequently can also cause this problem. An increased risk of air trapping with high respiratory rates may also potentially occur with the A/C ventilation.
· The A/C rate is the minimum number of full ventilator breaths the patient will receive. The actual respiratory rate is equal to the A/C rate plus any patient-triggered breaths per minute.
· This mode is used for patients who can initiate a breath but who have weakened respiratory muscles.

Intermittent Mandatory Ventilation (IMV) & Synchronous IMV (SIMV)
IMV
· IMV is the most commonly used modes of ventilation.
· In this mode the ventilator delivers a preset rate, tidal volume (or inspiratory pressure) and FiO2.
· The patient may also draw spontaneous breaths in-between mandatory breaths. Unlike A/C, breaths that the patient takes spontaneously do not trigger or cycle the ventilator.
· Patient-initiated breaths are completely spontaneous, neither assisted nor supported by the ventilator.

SIMV
· SIMV was developed as a result of the problem of high respiratory rates associated with A/C.
· SIMV delivers the preset volume or pressure and rate while allowing the patient to breathe spontaneously in between ventilator breaths. Each ventilator breath is delivered in synchrony with the patient’s breaths, yet the patient is allowed to completely control the spontaneous breaths.
· SIMV allows the patient to generate spontaneous breaths, volumes, and flow rates between the set breaths.
· SIMV is used as a primary mode of ventilation, as well as a weaning mode. During weaning, the preset rate is gradually reduced, allowing the patient to slowly regain breathing on his or her own.


Advantages
· Maintains respiratory muscle strength by avoiding muscle atrophy
· Decreases mean airway pressure
· Facilitates ventilator discontinuation – “weaning”
· Decreased chance of hyperventilation,
· Decreased atrophy of accessory muscles, and
· Improved distribution of gas throughout the lungs by the action of the diaphragm.
Disadvantages
· This mode may increase the work of breathing and respiratory muscle fatigue.
· In IMV mode the mechanical rate and spontaneous rate may asynchronous causing “stacking” and that may cause barotrauma or volutrauma
Spontaneous Modes OR Customized Adjuncts to Ventilator Modes
PEEP (Positive End Expiratory Pressure)
· According to its purest definition, the term PEEP is defined as positive pressure at the end of exhalation during either spontaneous breathing or mechanical ventilation. However, use of the term commonly implies that the patient is also receiving mandatory breaths from a ventilator.
· One method of improving the patient’s oxygenation without increasing the FiO2 is the use of PEEP. Basically, PEEP does not allow airway pressure to return to zero at the end of expiration.


· PEEP is not a mode of ventilation in itself. It is an adjunctive therapy added to other modes. It is intended to improve oxygenation, not to provide ventilation, which is the movement of air into the lungs followed by exhalation
· PEEP is added to increase functional residual capacity (FRC) and allow for a decrease in the FiO2. PEEP helps to prevent small airway and alveolar collapse, improves alveolar ventilation and may decrease the work of breathing (at low levels). PEEP facilitates oxygen diffusion at lower FiO2 levels, which is safer for the patient.
· PEEP of 5cm H2O pressure is referred to as “physiologic” PEEP because it is equivalent to the effect of the closed glottis. Therapeutic PEEP usually ranges from 10-30cm H2O in adults.
· PEEP is an effective therapy for disease processes involving atelectasis; it is a cornerstone of therapy for ARDS.
Disadvantage
· Decreased cardiac output with or without hypotension occurs because PEEP increases intra-thoracic pressure, which in turn decreases the venous return to the heart (preload).
· Potential volutrauma and barotrauma,
· Increased intracranial pressure and
· Potential loss of tidal volume
Continuous Positive Airway Pressure (CPAP)
· CPAP is similar to PEEP except that it works only for patients who are breathing spontaneously.
· CPAP is PEEP with no set rate on the ventilator. CPAP is primarily used as a mode of non-invasive mechanical ventilation. It is occasionally used in the final stages of ventilator weaning, but has minimal application for the mechanically ventilated patient.
· Patients on CPAP do not receive positive pressure breaths from the ventilator. All breaths are initiated and ended by the patient; tidal volumes and pressures are variable from breath to breath.
· CPAP can also be administered using a mask and CPAP machine for patients who do not require mechanical ventilation, but who need respiratory support; for example, patients with sleep apnea.
· CPAP aids in promotion of oxygenation in the same way PEEP does. It has no influence on ventilation.
Advantage
· Ventilator can monitor the patient’s breathing and activate an alarm if something undesirable occurs
· Helpful for improving oxygenation in patients with refractory hypoxemia and a low FRC
· CPAP setting is adjusted to provide the best oxygenation with the lowest positive pressure and the lowest FiO2

|
S.No. |
MODE |
FUNCTION |
CLINICAL USE |
|
1. |
Control Ventilation (CV) |
Delivers preset volume or pressure regardless of patient’s own inspiratory efforts |
Usually used for patients who are apneic |
|
2. |
Assist-Control Ventilation (A/C) |
Delivers breath in response to patient effort and if patient fails to do so within preset amount of time |
Usually used for spontaneously breathing patients with weakened respiratory muscles |
|
3. |
Synchronous Intermittent Mandatory Ventilation (SIMV) |
Ventilator breaths are synchronized with patient’s respiratory effort |
Usually used to wean patients from mechanical ventilation |
|
4. |
Pressure Support Ventilation (PSV) |
Preset pressure that augments the patient’s inspiratory effort and decreases the work of breathing |
Often used with SIMV during weaning |
|
5. |
Positive End Expiratory Pressure (PEEP) |
Positive pressure applied at the end of expiration |
Used with CV, A/C, and SIMV to improve oxygenation by opening collapsed alveoli |
|
6. |
Constant Positive Airway Pressure (CPAP) |
Similar to PEEP but used only with spontaneously breathing patients |
Maintains constant positive pressure in airways so resistance is decreased |
|
7. |
Independent Lung Ventilation (ILV) |
Ventilates each lung separately; requires two ventilators and sedation/paralysis |
Used for patients with unilateral lung disease or different disease process in each lung |
|
8. |
High Frequency Ventilation (HFV) |
Delivers small amounts of gas at a rapid rate (60-100 breaths/minute); requires sedation/paralysis |
Used for hemodynamic instability, during short-term procedures, or if patient is at risk for pneumothorax |
|
9. |
Positive End Expiratory Pressure (PEEP) |
Positive pressure applied at the end of expiration |
Used with CV, A/C, and SIMV to improve oxygenation by opening collapsed alveoli |
As mentioned earlier, the ventilator is designed to monitor many aspects of the patient’s respiratory status, and there are many different alarms that can be set to warn healthcare providers that the patient isn’t tolerating the mode or settings. The following are common ventilator alarms and their most frequent causes.
|
High Pressure Limit |
Low Pressure |
High Respiratory Rate |
Low Exhaled Volume |
|
· Secretions in ETT/airway or condensation in tubing · Kink in ventilator tubing · Patient biting on ETT · Patient coughing, gagging, or trying to talk · Increased airway pressure from bronchospasm or pneumothorax |
· Vent tubing not connected · Displaced ETT or tracheostomy tube |
· Patient anxiety or pain · Secretions in ETT/airway · Hypoxia · Hypercapnia |
· Vent tubing not connected · Leak in cuff or inadequate cuff seal · Occurrence of another alarm preventing full delivery of breath |
Books
1. Brunner LS, Suddarth DS, Smeltzer SCO. Brunner & Suddarth’s textbook of medical-surgical nursing. Philadelphia: Lippincott Williams & Wilkins; 2008. Page No. 739-754
2. Nettina SM, Lippincott Williams & Wilkins. Lippincott manual of nursing practice. Philadelphia: Wolters Kluwer Health : Lippincott Williams & Wilkins; 2010. Page No. 255-267
3. Longo DL, Harrison T. Harrison’s principles of internal medicine. New York, N.Y., [etc.]: McGraw-Hill Medical; 2012. Page No-
4. Colledge NR, Walker BR, Ralston S, Davidson S. Davidson’s principles and practice of medicine. Edinburgh; New York: Churchill Livingstone/Elsevier; 2010. Page No. 194-198
Web page
1. Adult Invasive Mechanical Ventilation.pdf [Internet]. [cited 2012 May 28]. Available from: http://www.mecriticalcare.net/downloads/mv/AdultInvasiveMechanicalVentilation.pdf
2. Adult Ventilation Management Online Nursing Continuing Education Course [Internet]. [cited 2012 May 28]. Available from: http://www.corexcel.com/courses/Vent_Web_Handout.pdf
3. Critical Care Nursing Theory - Mechanical ventilation [Internet]. [cited 2012 May 28]. Available from: http://www.philadelphia.edu.jo/academics/abatiha/uploads/Mechanical%20ventilation.pdf
4. Patient Education Series American Thoracic Society Mechanical Ventilation [Internet]. [cited 2012 May 28]. Available from: http://patients.thoracic.org/information-series/en/resources/mechanical-ventilation.pdf
5. Core Topics in Mechanical Ventilation [Internet]. [cited 2012 May 28]. Available from: http://www.csen.com/vent.pdf
6. Fundamentals of Mechanical Ventilation [Internet]. [cited 2012 May 28]. Available from: http://www.ventworld.com/resources/pdf/vwchat.pdf
7. Mechanical Ventilation Critical Care Clinic [Internet]. [cited 2012 May 28]. Available from: http://www.scribd.com/doc/25317501/Mechanical-Ventilation-Critical
8. Mechanical Ventilation for Nursing.ppt [Internet]. [cited 2012 May 28]. Available from: http://wwwappskc.lonestar.edu/programs/respcare/Missy%27s%20website/Mechanical%20Ventilation%20for%20Nursing.ppt
9. Mechanical ventilation Skills and techniques Update 2011 [Internet]. [cited 2012 May 28]. Available from: http://pact.esicm.org/media/Mechanical%20vent%201Feb2011%20final.pdf
10. Mechanical Ventilation.ppt [Internet]. [cited 2012 May 28]. Available from: http://home.cmcvellore.ac.in/upcoming/CME/ppt/Mechanical%20Ventilation.ppt
11. Mechanical Ventilation.ppt [Internet]. [cited 2012 May 28]. Available from: http://www.mcgill.ca/files/emergency/Mechanical_Ventilation.ppt
12. Modes of Ventilation ppt [Internet]. [cited 2012 May 28]. Available from: http://faculty.mdc.edu/pslocum/RET%202284%20Mod%203.0%20Modes%20of%20Ventilation.ppt
13. Nursing care of the mechanically ventilated patient: What does the evidence say? pdf [Internet]. [cited 2012 May 28]. Available from: http://eprints.qut.edu.au/33268/1/coyerdarticle%5B1%5D.pdf
14. Nursing Care Of The Ventilated Patient [Internet]. [cited 2012 May 28]. Available from: http://intensivecare.hsnet.nsw.gov.au/five/doc/nurse_care_V_swahs.pdf
15. Principle of Mechenical Ventilation [Internet]. [cited 2012 May 28]. Available from: http://www.cmia.org/images/ventilation.pdf
16. Chapter 82 - Mechanical Ventilation [Internet]. [cited 2012 May 28]. Available from: http://kemt.fei.tuke.sk/Predmety/KEMT537_LE/_materialy/09-Biomedical%20Engineering%20Handbook,%20The%20-Volumes%201%20%26%202/ch082.pdf
17. respiratory-failure-mechanical-ventilation.pdf [Internet]. [cited 2012 May 28]. Available from: http://www.thoracic.org/clinical/critical-care/clinical-education/respiratory-failure-mechanical-ventilation.pdf
18. Advances In Mechanical Ventilation [Internet]. [cited 2012 May 28]. Available from: http://www.newportnmi.com/FileDownloads/GENERAL-tobinmechvent.pdf
19. Standard of Practice: Care of the Mechanically Ventilated Patient [Internet]. [cited 2012 May 28]. Available from: http://www.cc.nih.gov/ccmd/cctrcs/pdf_docs/Ventilator%20Management/01-SOP-Carof%20the%20Mech.pdf
20. Invasive Mechanical Ventilation ppt [Internet]. [cited 2012 May 28]. Available from: http://home.cmcvellore.ac.in/upcoming/CME/ppt/Invasive%20Mechanical%20Ventilation.ppt
21. Management of the mechanically ventilated. Patient in the emergency department [Internet]. [cited 2012 May 28]. Available from: https://notendur.hi.is/thorsj/tasota/ED_MV.pdf
22. Mechanical Ventilation: A Review and Update for Clinicians [Internet]. [cited 2012 May 28]. Available from: http://seminmedpract.com/pdf/hp_dec99_vent.pdf
23. How to Withdraw Mechanical Ventilation [Internet]. [cited 2012 May 28]. Available from: http://www.aacn.org/WD/CETests/Media/CI1841.pdf
24. Mechanical ventilation: Weaning and extubation [Internet]. [cited 2012 May 28]. Available from: http://www.opus12.org/uploads/O12-SCI-V01-N02-P13.pdf
25. Withdrawal of Ventilatory Support from the Dying Adult Patient [Internet]. [cited 2012 May 28]. Available from: http://jso.imng.com/jso/journal/articles/0203283.pdf
Geek Squad Protection goes above and beyond the manufacturer's warranty to extend your coverage and protect your purchase.
ReplyDeletegeek squad chat
geek squad tech support
geek squad chat
geek squad tech support
geek squad appointment
geek squad support
geek squad chat
Nice to read it
ReplyDeleteHey what a brilliant post I have come across and believe me I have been searching out for this similar kind of post for past a week and hardly came across this. Thank you very much and will look for more postings from you. https://europa-road.eu/hu/kombajn-szallitas-mezogazdasagi-gep-szallitas.php
ReplyDeleteGreat Blog!Thank you for sharing the information.
ReplyDeleteDownload Indian Doctors Network and be part of fastest growing doctors network.
very nice post will you please mail it to me
ReplyDeleteWe're covering it all. Do you need a ride to a doctor or a grocery store?
ReplyDeletesenior companion care There's no problem! Our carers are here to help you with your daily appointments.
Very good 👍
ReplyDeleteAmazing content with extremely useful information. We are waiting for your next blog.
ReplyDeleteBaby boy names starting with the letter A
For NORCET online coaching in Yamuna Nagar, Haryana, Mantram Nursing Academy offers live classes, subject-focused lessons, and regular quizzes to boost students’ confidence for the NORCET exam.
ReplyDeleteNORCET Online Coaching in Yamuna Nagar Haryana